Prognostic Implications of Staging Right Heart Failure in Patients With Significant Secondary Tricuspid Regurgitation
JACC: Heart Failure Research Article
Aug 01, 2020: 8 (8),
10.1016/j.jchf.2020.02.008
Central Illustration

Objectives
The purpose of this study was to evaluate the prognostic value of staging right heart failure (RHF) in patients with significant secondary tricuspid regurgitation (TR).本研究的目的是评估右心衰竭(RHF)分期对严重继发三尖瓣反流(TR)患者的预后价值。
Background
Right ventricular dysfunction (RVD), defined as tricuspid annular plane systolic excursion <17 mm and clinical signs of RHF, defined as New York Heart Association functional class ≥II, peripheral edema, or use of diuretics, do not always coincide in patients with significant secondary TR and may have different prognostic implications.右心室功能不全(RVD)定义为三尖瓣环平面收缩偏移<17 mm,RHF的临床症状,定义为纽约心脏协会功能分级≥II级,周围水肿,或使用利尿剂,在有明显继发性TR的患者中并不总是一致的,并且可能有不同的预后影响。
Methods
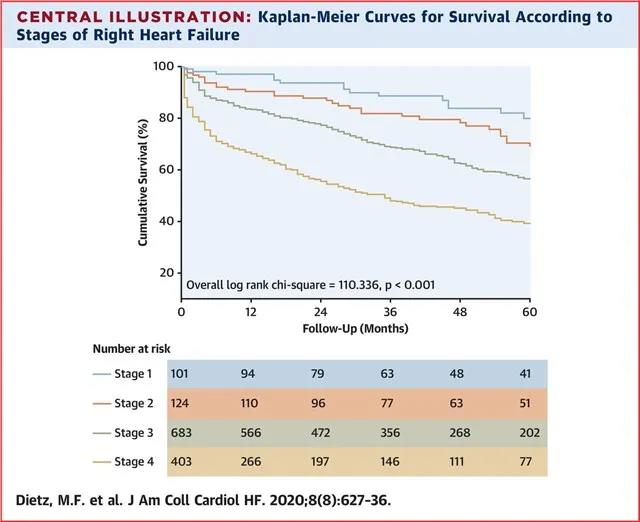
A total of 1,311 patients with significant secondary TR (median age: 71 [interquartile range: 62 to 78] years; 50% male) were divided into 4 RHF Stages according to the presence or absence of RVD and clinical signs of RHF: Stage 1 was defined as no RVD and no signs of RHF; Stage 2 indicated RVD but no signs of RHF; Stage 3 included RVD and signs of RHF; Stage 4 was defined as RVD and refractory signs of RHF at rest. Five-year mortality rates were compared across the 4 Stages of RHF, and the independent associates of mortality were identified by using multivariate Cox proportional hazards models.共有1311例继发性TR患者(中位年龄:71岁[四分位间距:62-78]岁;50%男性)根据是否存在RVD和RHF的临床症状分为4个RHF分期:1期为无RVD,无RHF征象;2期为RVD但无RHF征象;RHF期和RHF期的标志分别为RHF期和RHF期。比较了4个阶段RHF的5年死亡率,并用多元Cox比例风险模型确定了死亡率的独立关联。
Results
A total of 101 patients (8%) were classified as Stage 1, 124 (10%) as Stage 2, 683 (52%) as Stage 3, and 403 (31%) as Stage 4. Patients in higher Stages of RHF had more comorbidities and worse renal and left ventricular systolic function. Cumulative 5-year survival was 54%. RHF Stages 3 and 4 were independently associated with increased mortality compared to Stage 1 (hazard ratio: 2.110 [95% confidence interval (CI): 1.163 to 3.828] and 3.318 [95% CI: 1.795 to 6.133], respectively).共有101例(8%)患者被分为1期,124例(10%)分为2期,683例(52%)分为3期,403例(31%)分为4期。晚期RHF患者合并症多,肾、左室收缩功能差。累积5年生存率为54%。与1期相比,RHF 3期和4期与死亡率增加独立相关(危险比:2.110[95%可信区间:1.163-3.828]和3.318[95%CI:1.795-6.133])。
Conclusions
In patients with significant secondary TR, higher Stages of RHF are independently associated with all-cause mortality at long-term follow-up.在有明显继发性TR的患者中,在长期随访中,RHF的高阶段性与全因死亡率独立相关。
Footnotes
Supported by an unrestricted research grant from Edwards Lifesciences (IISUSTHV2018017) and by research grants from Abbott Vascular, Bioventrix, Medtronic, Biotronik, Boston Scientific, and GE Healthcare to the Department of Cardiology of the Leiden University Medical Center. Drs. Bax and Ajmone Marsan have received speaker fees from Abbott Vascular. Dr. Delgado has received speaker fees from Abbott Vascular, Medtronic, Edwards Lifesciences, and GE Healthcare. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the JACC: Heart Failure .
References
1. T.M. Gorter, D.J. van Veldhuisen, J. Bauersachs. Right-heart dysfunction and failure in heart failure with preserved ejection fraction: mechanisms and management. Position statement on behalf of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2018;20:16-37. doi:2. C.W. Yancy, M. Jessup, B. Bozkurt. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. JACC2013;62:e147-e239. doi: 10.1016/j.jacc.2013.05.0193. F. Haddad, R. Doyle, D.J. Murphy, S.A. Hunt. Right Ventricular Function in Cardiovascular Disease, Part II: Pathophysiology, Clinical Importance, and Management of Right Ventricular Failure. Circulation 2008;117:1717-1731. doi: 10.1161/CIRCULATIONAHA.107.6535844. A.A. Kammerlander, B.A. Marzluf, A. Graf. Right Ventricular Dysfunction, But Not Tricuspid Regurgitation, Is Associated With Outcome Late After Left Heart Valve Procedure. JACC 2014;64:2633-2642. doi: 10.1016/j.jacc.2014.09.0625. W.A. Zoghbi, D. Adams, R.O. Bonow. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American Society of Echocardiography developed in collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr 2017;30:303-371. doi:6. R.M. Lang, L.P. Badano, V. Mor-Avi. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2015;16:. doi: 10.1093/ehjci/jev0147. L.G. Rudski, W.W. Lai, J. Afilalo. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr2010;23:685-713. doi: 10.1016/j.echo.2010.05.0108. P. Lancellotti, C. Tribouilloy, A. Hagendorff. Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2013;14:. doi: 10.1093/ehjci/jet1059. H. Baumgartner, J. Hung, J. Bermejo. Recommendations on the echocardiographic assessment of aortic valve stenosis: a focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography.J Am Soc Echocardiogr 2017;30:372-392. doi:10. J. Nath, E. Foster, P.A. Heidenreich. Impact of tricuspid regurgitation on long-term survival. JACC 2004;43:405-409. doi: 10.1016/j.jacc.2003.09.03611. N. Wang, J. Fulcher, N. Abeysuriya. Tricuspid regurgitation is associated with increased mortality independent of pulmonary pressures and right heart failure: a systematic review and meta-analysis. Eur Heart J 2019;40:476-484. doi:12. C.J. Zack, E.A. Fender, P. Chandrashekar. National Trends and Outcomes in Isolated Tricuspid Valve Surgery. JACC2017;70:2953-2960. doi: 10.1016/j.jacc.2017.10.03913. E.A. Fender, C.J. Zack, R.A. Nishimura. Isolated tricuspid regurgitation: outcomes and therapeutic interventions. Heart2018;104:. doi: 10.1136/heartjnl-2017-31158614. M. Hamandi, R.L. Smith, W.H. Ryan. Outcomes of isolated tricuspid valve surgery have improved in the modern era. Ann Thorac Surg 2019;108:11-15. doi:15. Y.J. Kim, D.A. Kwon, H.K. Kim. Determinants of surgical outcome in patients with isolated tricuspid regurgitation.Circulation 2009;120:. doi: 10.1161/CIRCULATIONAHA.109.84944816. N.F. Voelkel, R.A. Quaife, L.A. Leinwand. Right Ventricular Function and Failure: Report of a National Heart, Lung, and Blood Institute Working Group on Cellular and Molecular Mechanisms of Right Heart Failure. Circulation 2006;114:1883-1891. doi: 10.1161/CIRCULATIONAHA.106.63220817. M.F. Dietz, E.A. Prihadi, P. van der Bijl. Prognostic implications of right ventricular remodeling and function in patients with significant secondary tricuspid regurgitation. Circulation 2019;140:836-845. doi:18. M. Taramasso, M. Gavazzoni, A. Pozzoli. Tricuspid regurgitation: predicting the need for intervention, procedural success, and recurrence of disease. J Am Coll Cardiol Img 2019;12:605-621. doi:19. L.A. Schwartz, Z. Rozenbaum, E. Ghantous. Impact of right ventricular dysfunction and tricuspid regurgitation on outcomes in patients undergoing transcatheter aortic valve replacement. J Am Soc Echocardiogr 2017;30:36-46. doi:20. N. Bar, L.A. Schwartz, S. Biner. Clinical outcome of isolated tricuspid regurgitation in patients with preserved left ventricular ejection fraction and pulmonary hypertension. J Am Soc Echocardiogr 2018;31:34-41. doi:21. Y. Topilsky, J.M. Inojosa, G. Benfari. Clinical presentation and outcome of tricuspid regurgitation in patients with systolic dysfunction. Eur Heart J 2018;39:3584-3592. doi:22. U. Sartipy, U. Dahlstrom, M. Fu, L.H. Lund. Atrial fibrillation in heart failure with preserved, mid-range, and reduced ejection fraction. J Am Coll Cardiol HF 2017;5:565-574. doi:23. R. Nasser, L. Van Assche, A. Vorlat. Evolution of functional mitral regurgitation and prognosis in medically managed heart failure patients with reduced ejection fraction. J Am Coll Cardiol HF 2017;5:652-659. doi:24. G. Benfari, C. Antoine, W.L. Miller. Excess mortality associated with functional tricuspid regurgitation complicating heart failure with reduced ejection fraction. Circulation 2019;140:196-206. doi:25. T.G. Di Salvo, M. Mathier, M.J. Semigran, G.W. Dec. Preserved right ventricular ejection fraction predicts exercise capacity and survival in advanced heart failure. JACC 1995;25:1143-1153. doi: 10.1016/0735-1097(94)00511-N26. B.J. Baker, M.M. Wilen, C.M. Boyd, H. Dinh, J.A. Franciosa. Relation of right ventricular ejection fraction to exercise capacity in chronic left ventricular failure.. Am J Cardiol 1984;54:596-599. doi: 10.1016/0002-9149(84)90256-X27. S.J. Pocock, C.A. Ariti, J.J. McMurray. Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J 2013;34:. doi: 10.1093/eurheartj/ehs337